
Oculo-orbital prosthetics with hydroxyapatite nanocomposite materials
Doctoral Thesis Summary
Doctoral student: Grădinaru Sînziana Luminița
Coordinator: Prof.Univ.Dr Liliana Mary Voinea
INTRODUCTION
In ocular pathology, there are situations in which preserving the eyeball is impossible, requiring radical surgery, the loss of an organ having both a psychological impact on the patient and a socio-economic impact, requiring prosthetics of the remaining cavity for a satisfactory result. A patient facing the reality of a permanent loss of an eyeball requires medical support, psychological rehabilitation and social reintegration, in order to achieve a normal quality of life. When an eye is removed, more frequently after trauma or infection, but also from congenital diseases or cancer, an orbital implant is used to fill the volume in the orbit (the bony cavity around the eye), so as to maintain the natural appearance of the orbit and to provide support for the artificial eye (ocular prosthesis).
The artificial eye has always been a goal, with attempts to create one involving the most unusual materials: glass, gold, silver, wool, rubber, cartilage, bone, fat, magnet, silicon, cork, titanium, acrylates, catgut, agar, asbestos, cellulose, paraffin, sponge, polymethylmethacrylate (PMMA), polyethylene, and hydroxyapatite. The first generation of orbital implants could not give the artificial eye a natural movement. The natural appearance and movement of the artificial eye was achieved by using a natural material: ocean coral, whose porous structure is similar to that of human bone, which allows the growth of its own fibrovascular material inside the implant and solidifies the implant to the adjacent tissues.
In 1985, Dr. Arthur Perry made the first porous orbital implant from a reef coral whose structure was changed from calcium carbonate to calcium phosphate (mainly hydroxyapatite – HA) by a hydrothermal reaction that simultaneously removed proteins and residual materials. Implant design has progressed significantly in recent years with the use of porous devices, which have reduced complications and improved cosmetic appearance.
But these advantages come after a long period of healing, sometimes with less than satisfactory results, complications and prolonged hospitalization. Also, the patient’s reintegration into society takes longer, many of them have to wait for the vascularization of the implant, then undergo other new surgical procedures for the second stage of drilling. In the case of mid-facial trauma, patients endure not only the physical consequences, but also face the reality of possible permanent deformities with significant consequences on the psychological status.
Mid-facial trauma is accompanied by edema and ecchymosis of the soft tissues, subconjunctival hemorrhage, diplopia, iritis, retinal edema, ptosis, enophthalmos, paresis of the ocular muscles, mechanical restriction of ocular movements and nasolacrimal dysfunction. The main dysfunctions that patients have to deal with are: persistent diplopia caused by ineffective muscle movements caused by fractures, poor positioning of the eyeball, sensory disturbances on the areas innervated by the branches of the trigeminal nerve and mastication dysfunctions. Patients who suffer facial trauma are seriously affected psychologically, even those who apparently accept their appearance.
Physiognomy modified at a young age and binocular appearance matter in a world where people like eye contact, and impaired eye motility can diminish social activities and interpersonal contacts. Patients become more withdrawn, talk and laugh less to mask the change in physiognomy. Most cases require reconstruction of the orbital floor to maintain the position of the eyeball and restore the shape of the orbit. The reason for this reconstruction is that the bone walls have suffered comminuted fractures and/or have missing bone fragments. Therefore, reconstruction of the missing bone is preferred over reduction of bone fragments. This can be accomplished using a variety of materials. There are few anatomical regions in the human body that are so controversial regarding the use of appropriate materials for fracture reduction, hence the trend of the last 10 years of research in the field to find the ideal prosthetic material.
The general objective of the present work is to provide new solutions for an ocular prosthesis and orbital fracture repair material and to implement new interventional strategies at the oculo-orbital level. The concern to obtain rapid benefits for patients became my main objective during my PhD: the design and development of a new conceptual type of ocular implant by approaching nanotechnology, which will allow the creation of a skeleton with a higher rate of vascular proliferation for the replacement of the ocular content in the scleral sac, so that the waiting time for the final prostheses is shortened and the integrity of the eyelid is maintained, as well as a nanostructured hydroxyapatite skeleton for bone reconstruction in the case of orbital fractures. Since this thesis was partially carried out within the PARTNERSHIP project “PN-II-PT-PCCA-2013-4-0584- New ocular implant with high biocompatibility and proliferation rate (ORBIMPLANT)”, funded by UEFISCDI – EXECUTIVE UNIT FOR FINANCING HIGHER EDUCATION, RESEARCH, DEVELOPMENT AND INNOVATION, would like to thank Professor Liliana Voinea, the coordinator of this project, and her partners, especially Eng. Dr. Roxana Mioara Piticescu and Eng. Dr. Mădălina Popescu from the Institute of Non-Ferrous and Rare Materials (IMNR) for the guidance provided during my doctoral training.
Thesis structure
The thesis consists of two parts, one of which is of general interest (consisting of chapters 1-4) in which are presented:
– notions regarding the anatomy of the eyeball and its appendages with emphasis on the osteology of the orbit – elements of imaging applicable to the pathology of the eyeball, orbit and adnexa; – a chapter related to the indications of oculo-orbital prosthesis, both in ophthalmological interventions – enucleation and evisceration and in interdisciplinary interventions – ophthalmology, neurosurgery and oral and maxillofacial surgery to restore the walls of the orbit. consisting of five studies, three of which are clinical studies and two studies of fundamental research in the animal model. Chapter 10 is dedicated to the general conclusions of the thesis.
The thesis contains a total of 40 figures and graphs, a number of 23 tables and 270 bibliographical references. Of the figures and tables, only a part are included in this summary.
COMPARATIVE STUDY OF INTEGRATED IMPLANTS VERSUS NON-INTEGRATED IMPLANTS IN EVISCERATED PATIENTS
Study Objectives
Taking into account the important impact on the patient’s physiognomy of a surgical intervention aimed at removing the contents of the eyeball for various conditions, often as a final option after a long suffering, it is easy to conclude that the postoperative aesthetic aspect will be decisive in achieving the best possible quality of life for an already suffering patient.
A considerable proportion of patients present to the ophthalmologist after a period of considerable discomfort, and another large part end up in a situation of post-traumatic evisceration of the globe, so that the management of these cases becomes difficult and delicate to the same extent. Despite numerous publications on this topic, the conduct regarding prosthetics still remains in an unclear area, which does not yet allow the development of standard diagnostic and treatment guidelines.
The present study aims to qualitatively analyze two types of ocular implants, comparing evisceration surgeries and analyzing their therapeutic efficacy and success in terms of biocompatibility and frequency of postoperative complications.
The present paper presents a clinical, cohort, retrospective, non-randomized, comparative study analyzing patients undergoing evisceration between January 2009 and December 2013. The surgical approach was followed by the implantation of a hydroxyapatite implant (coraline or synthetic) or a non-integrated implant (acrylic or silicone) in the scleral sac. The study followed the provisions of the Helsinki Convention on patients’ rights.
Results
The present study considered a sample of 90 subjects with integrated or non-integrated implants who underwent evisceration surgery.
The descriptive characteristics of the sample are presented below:
The studied sample includes subjects of both sexes, with males accounting for 55.6% and females accounting for 44.4%.
It is found that the average age of the individuals in the sample is 56.41 years. The subjects’ age deviates from the mean by plus or minus 19.58 years. The mode (modal value) is multiple and has the lowest value of 57 years.
This means that the most frequently encountered age in the patients in the sample was 57 years. The minimum age is 20 years, while the maximum age is 93 years.
We observe that we have a negative asymmetric curve, slightly tilted to the right (Skewness coefficient -0.252), with more extreme values to the left and platykurtic (Skewness coefficient -0.892), flatter than a normal distribution, with more values dispersed over a larger interval around the mean. The explanation for this distribution is given by a higher number of eye traumas that are more common in the male population compared to the female population, who opted for surgical intervention most frequently to improve the cosmetic appearance.
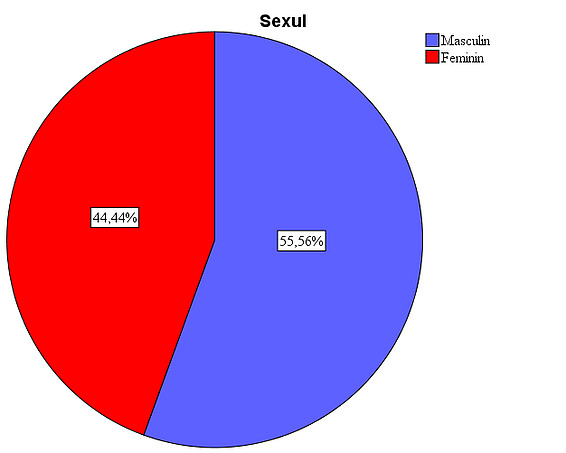
Figure 1: Gender distribution in the study. The presence of a larger number of male patients is due to the large number of eviscerations after ocular trauma, a pathology more frequently encountered in males (33 cases). The implant types were used in a relatively equal proportion: in 26.7% of patients the silicone implant was used, in 25.6% the synthetic hydroxyapatite implant, in 24.4% the acrylic implant, and in 23.3% the natural hydroxyapatite implant.
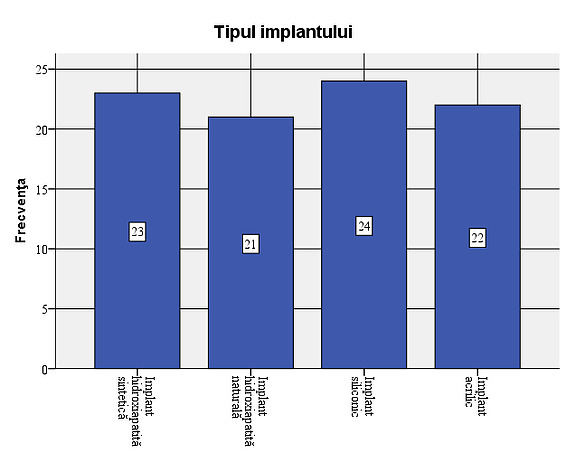
Figure 2: Types of implants used in the sample In 15 of the patients studied (16.7%), complications were observed: 5 cases of infections, 13 cases with extrusions and 2 cases with dehiscence. Out of the total of 15 cases with complications, extrusion occurred in 86.7%. Considering that all cases of infection were followed by extrusion, the situation of complications that occurred is as follows: 8 cases (8.9% of the total number of patients studied) with extrusion only, 5 cases (5.6%) of infection followed by extrusion and 2 cases (2.2%) with dehiscence. In most of the cases with complications, the association of infection with extrusion occurs, dehiscence not being associated with extrusion or infection.
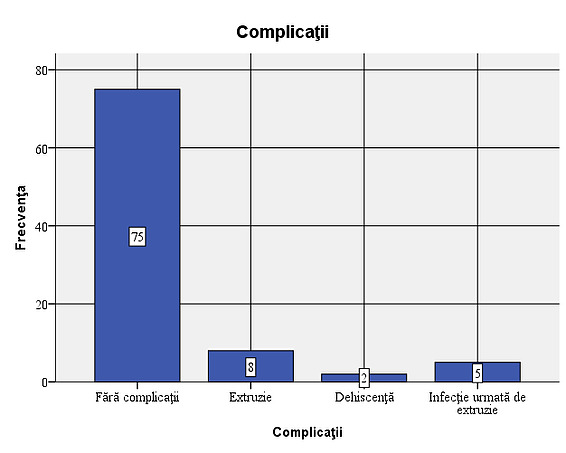
Figure 3: Frequency of complications – 8 cases (8.9% of the total patients studied) with extrusion only, 5 cases (5.6%) of infection followed by extrusion and 2 cases (2.2%) with dehiscence.
Objective verification: Existence of a link between the type of implant used and the presence of complications
Although it is observed that dehiscence occurred only in cases of hydroxyapatite implants, the very small number of cases prevents us from showing that this type of complication occurs more frequently in the case of these implants.
If we refer only to the individuals in the sample who experienced complications, the results obtained from the application of the chi-square test also show a statistically insignificant difference (χ2=11.750; df=6, p=0.068) between patients with different types of implants in terms of the presence of certain complications, confirming the conclusions shown previously, that is, there is no statistically significant relationship between the type of implant used and the occurrence of a certain type of complication.
Discussion
From the point of view of biocompatibility, all the tested materials offer the patient a good general rehabilitation, however, the hydroxyapatite implant, whether synthetic or coralline, offers a series of advantages that include a lower incidence of implant extrusion and better resistance to infections. Shields et al demonstrate in 3 consecutive papers on a large number of cases 1 that the presence of conjunctival dehiscence and exposure of the hydroxyapatite implant is reduced. Although acrylic and silicone implants have the added advantage of low cost and immediate availability, there is a higher rate of infection followed by extrusion, observed when considering cases with complications, associated complications requiring surgical reintervention.
Conclusions
The results obtained helped us to conclude the following:
- The studied sample includes subjects of both sexes, with males accounting for 55.6%, while females accounting for 44.4%, explained by the high rate of ocular trauma in male patients
- The average age of the people in the sample is 56.41 years. The minimum age is 20 years, while the maximum age is 93 years, explained on the one hand by the more frequent cosmetic surgical interventions in the first decades of life and the presence of neovascular glaucoma, which frequently involves a long period of illness in people in the 7th-8th decade of life.
- The types of implant were used in a relatively equal proportion: in 26.7% of the patients the silicone implant was used, in 25.6% the synthetic hydroxyapatite implant (FCI3), for 24.4% the acrylic implant (PMMA), and for 23.3% the natural hydroxyapatite implant (Bio-Eye);
- In 15 of the patients studied (16.7%) complications were observed: 5 cases of infections, 13 cases of extrusions and 2 cases of dehiscence. Considering that all cases of infection were followed by extrusion, the situation of complications that occurred is as follows: 8 cases (8.9% of the total number of patients studied) with extrusion only, 5 cases (5.6%) of infection followed by extrusion and 2 cases (2.2%) with dehiscence;
Although it is observed that dehiscence occurred only in the cases of hydroxyapatite implants, the very small number of cases prevents us from concluding that this type of complication occurs more frequently in the case of these implants. This could be explained by the fact that implantation in the scleral sac offers protection from infection and wound dehiscence. On the other hand, there is a greater number of associated complications (infection followed by extrusion) in the case of acrylic and silicone implants, which confer a higher degree of severity to these types of complications, which subsequently require a new surgical intervention to re-prosthetize the anophthalmic cavity. I believe that the choice of the type of implant, although it comes after a process of informing the patient, must also include a cost-effectiveness analysis, weighing up the possibility of new surgical re-interventions, especially in the young population.
COMPARATIVE STUDY OF INTEGRATED VERSUS NON-INTEGRATED IMPLANTS IN ENUCLEATED PATIENTS
Study objective
The present study aims to qualitatively analyze two types of integrated and non-integrated ocular implants, comparing surgical interventions for enucleation of the eyeball and analyzing their therapeutic efficacy and success in terms of biocompatibility and frequency of postoperative complications.
The present paper presents a clinical, cohort, retrospective, non-randomized, comparative study analyzing patients undergoing enucleation between January 2004 and December 2011. The surgical approach was followed by the implantation in the anophthalmic cavity of a hydroxyapatite implant (coraline or synthetic) or a non-integrated implant (acrylic or silicone).
Results
The descriptive characteristics of the sample are presented below: It is found that the average age of the people in the sample is 48.07 years. The age of the subjects deviates from the average by plus or minus 19.73 years. The mode (modal value) is multiple and has the lowest value of 28 years. The minimum age is 4 years, while the maximum age is 79 years. The most used implants in the patients studied were silicone ones (26.1% of the total cases), closely followed by acrylic ones (23.9%), those with synthetic hydroxyapatite (20.5%) and those with natural hydroxyapatite (17%). Implants with mixed natural hydroxyapatite (9.1% of cases) and those with mixed synthetic hydroxyapatite (3.4%) were also used.
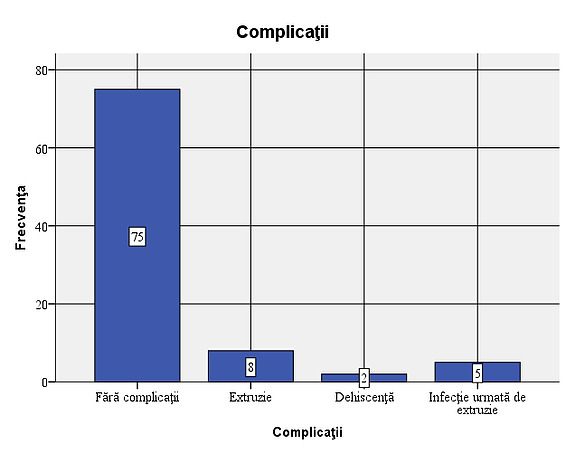
Figure 4: Frequency of complications in the studied group – 3 cases (3.4%) with dehiscence, 8 cases (9.1%) with extrusions and 5 cases (5.7%) of infection followed by extrusion. The association of the two types of complications – infection and extrusion gives additional gravity to the first.
Verification of the objective: Existence of a link between the type of implant used and the presence of complications
The bivariate Chi-square test (χ2) indicated the lack of a significant difference between the types of implants used and the occurrence of certain complications (χ2=24.769; df=15, p=0.054). Considering the value of the significance level obtained and which is very close to the conventional threshold of 0.05, I believe that we should not ignore the veracity of the research hypothesis, namely the existence of a relationship between the type of implant used and the occurrence of certain complications. Corroborating the data in the cross-tabulation below, it is observed that dehiscence occurs only in cases of hydroxyapatite implants, but their number is small, while extrusion cases occur in an overwhelming proportion only in the case of acrylic and silicone implants.
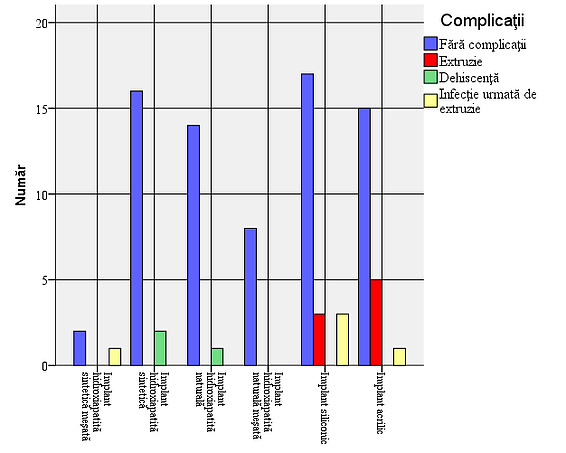
Figure 5: Frequency of complications depending on the type of implant. In the case of integrated implants, the complication rate is low, but a higher incidence of infection followed by extrusion is observed in relation to the number of cases in mixed synthetic hydroxyapatite implants. In non-integrated implants, the rate of severe complications is higher.
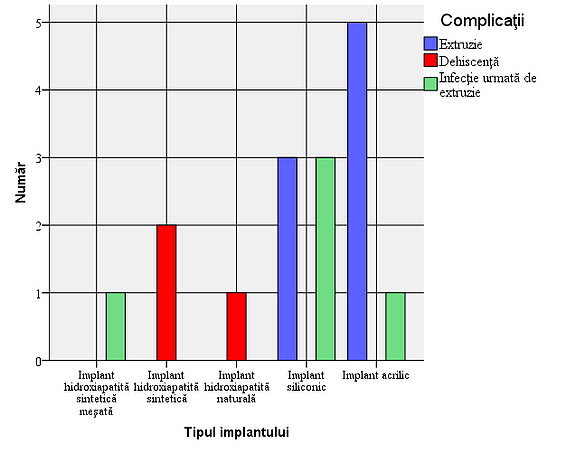
Figure 6: Type of complications depending on the type of implant: It is observed that dehiscence occurs only in cases of hydroxyapatite implants, but their number is small, while extrusion cases occur in an overwhelming proportion only in the case of acrylic and silicone implants
Taking into account strictly the cases with complications, the results obtained show a statistically significant difference (χ2=19.867; df=8, p=0.011) between the types of implants used in terms of the occurrence of certain complications, thus confirming the conclusions above.
The value of Cramer’s V coefficient (Cramer’s V=0.788) indicates a high intensity relationship between the two factors: the types of implants used and the types of complications that occurred.
Discussions
Following the analysis of the study results, we can say that dehiscence occurs only in cases of hydroxyapatite implants, but their number is small, while extrusion cases occur in an overwhelming proportion only in the case of acrylic and silicone implants. Data from the literature confirm the higher incidence of extrusion-type complications of non-integrated implants, also explained by the tendency to constrict the anophthalmic cavity 2. Dehiscence is an important complication that requires reintervention to cover the defect (in the cases presented in the study, autotransplantation was practiced by covering with buccal mucosa), its occurrence being also explained by the fact that the integrated implant and the removable prosthesis allow the application of higher shear forces in mechanically weak areas, which are additionally required and where a healing process has already occurred, i.e. at the level of the conjunctival sutures and Tenon’s capsule. Conclusions The results obtained helped us to conclude the following:
- The studied sample includes subjects of both sexes, in relatively equal proportions, male representatives being in the proportion of 52.3%, while female representatives in the proportion of 47.7%, a proportion explained by the high rate of surgical interventions post-traumatic, more common in the male population.
- The average age of the people in the sample is 48.07 years. The minimum age is 4 years, while the maximum age is 79 years, extreme ages given by the incidence of malignant ocular pathology at this age (retinoblastoma in children, respectively malignant melanoma in the adult population)
- The most used implants in the patients studied were silicone ones (26.1% of all cases), closely followed by acrylic ones (23.9%), those with synthetic hydroxyapatite (20.5%) and those with natural hydroxyapatite (17%). Implants with mixed natural hydroxyapatite (9.1% of cases) and those with mixed synthetic hydroxyapatite (3.4%) were also used;
- Complications were observed in 16 patients (18.2%): 5 cases of infection, 13 of extrusion and 3 with dehiscence. All cases of infection were followed by extrusion, so we have 3 cases (3.4%) with dehiscence, 8 cases (9.1%) with extrusion and 5 cases (5.7%) of infection followed by extrusion;
- It is observed that dehiscence occurs only in cases of hydroxyapatite implants, but their number is small, while cases of extrusion occur in an overwhelming proportion only in the case of acrylic and silicone implants. The conclusions are confirmed if we consider only cases with complications.
COMPARATIVE STUDY OF TOPOGRAPHIC MEASUREMENTS OF THE EYELIDS AND ORBITS IN PATIENTS EVISCERATED WITH HYDROXYAPATITE IMPLANTS VERSUS PMMA
Objective of the study: Aging leads to laxity of orbital tissues and fat that contributes to the etiology of many eyelid conditions such as ectropion, entropion, dermatochalasis or blepharoptosis. These changes can affect the position of the eyelids, eyeball or eyebrows and surgical interventions can contribute to the final cosmetic appearance especially after evisceration and prosthetics of the anophthalmic cavity. Tyers and Collin first described in 1982 the insufficient cavity syndrome characterized by a deep superior sulcus, enophthalmic appearance, ptosis of the upper eyelid and malposition of the lower eyelid, which can occur especially in the case of cavities insufficiently filled by prosthetics 2. Through this study, I want to make a comparison between the 2 types of implants regarding the existence of aesthetic differences between the prosthetic eye and the healthy eye 4 years after the prosthesis, the existence of aesthetic differences between the prosthetic eye with an acrylic implant and the one with a hydroxyapatite implant 4 years after the prosthesis and the existence of a correlation between age and the aesthetic appearance of the prosthetic eye 4 years after the prosthesis. The present paper presents a clinical, cohort, retrospective, non-randomized, comparative study analyzing patients undergoing evisceration between January 2006 and December 2010. The surgical approach was followed by the implantation in the anophthalmic cavity of a coralline hydroxyapatite implant or a non-integrated implant (PMMA). Investigated population The present study considered a sample of 43 subjects with ocular implants. The descriptive characteristics of the sample are presented below: Gender Analyzing the structure of the sample according to the sex of the subjects, it is observed that men have a share of 65.1%, while women represent only 34.9%.
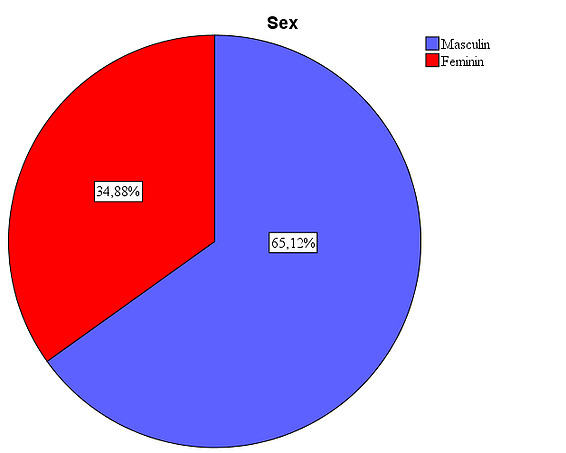
Figure 7: Gender distribution of the sample: , it is observed that men have a share of 65.1%, while women represent only 34.9%. Age: Looking at the sample from the perspective of the subjects’ age, it is found that their average age is 57.42. The age deviates from the average by plus or minus 5.36 years. The modal value (Mode) shows us that the age of 58 was the most common among the people in the sample.
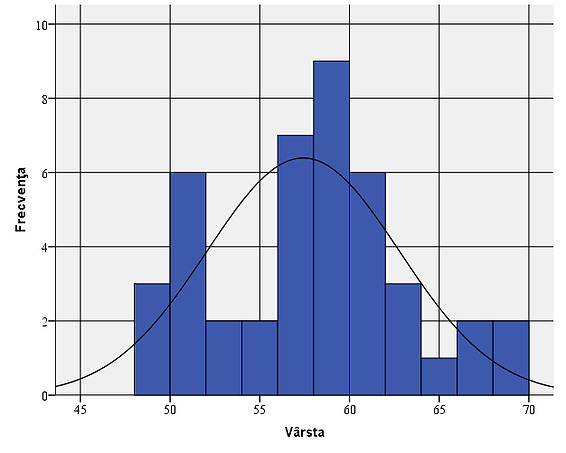
Figure 8: Age variation within the sample:, it is found that their average age is 57.42. The age deviates from the average by plus or minus 5.36 years. The acrylic implant was used in 23 of the patients studied (53.5%), while the natural hydroxyapatite implant was used in 20 of the patients (46.5%).
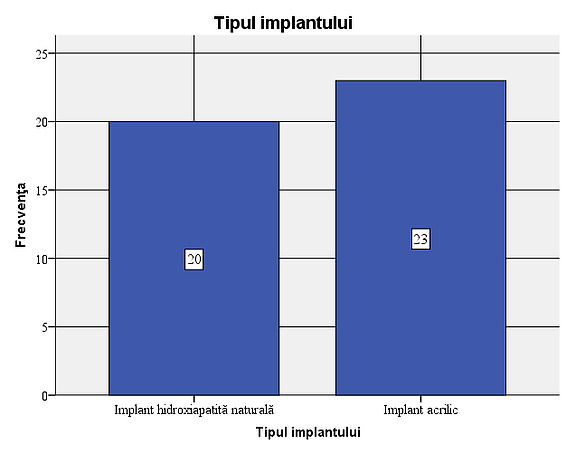
Figure 9: Type of implants used in the sample: 23 of the patients studied (53.5%) had a non-integrated acrylic implant (PMMA), while the natural hydroxyapatite implant was used in 20 of the patients (46.5%).
Verification of objective 1: Existence of aesthetic differences between the prosthetic eye and the healthy eye 4 years after the prosthesis.
To compare the aesthetic level of the operated eye with the level of the healthy eye 4 years after the prosthesis, we used the t-test for dependent samples (pairs). The test was applied to compare the palpebral aperture, the horizontal fissure and the exophthalmometry result. The average palpebral aperture in the operated eye was 12.05, while in the healthy eye it was 10.19. The horizontal fissure in the operated eye had an average of 26.72, while in the healthy eye it had an average of 29.12. Regarding exophthalmometry, in the operated eye the average value was 11.05, while in the healthy eye it was 13.88. It is found, with regard to each factor, that the means obtained differ significantly: for palpebral aperture (t=8.469; df=42; p<0.001), for the horizontal fissure (t=-11.811; df=42; p<0.001), and for exophthalmometry (t=-12.445; df=42; p<0.001) The results obtained show significant differences in the aesthetic appearance between the operated and the healthy eye 4 years after the prosthesis.
Paired Samples Statistics
MeanNStd. DeviationStd. Error MeanPair 1 Palperal aperture operated eye 12.05431.174.179 Palperal aperture normal eye 10.1943.732.112 Pair 2 Horizontal fissure operated eye 26.72432.027.309 Horizontal fissure normal eye 29.12431.434.219 Pair 3 Exophthalmometry operated eye 11.05431.877.286 Exophthalmometry normal eye 13.88431.051.160
Table 1: t-test for dependent samples (pairs). The test was applied to compare palpebral aperture, horizontal fissure and exophthalmometry result.
Verification of objective 2: Existence of aesthetic differences between the eye prosthetically implanted with an acrylic implant and the one prosthetically implanted with a hydroxyapatite implant 4 years after the prosthesis. To evaluate the aesthetic point of view of the ocular prostheses 4 years after the operation, we resorted to calculating the differences between the healthy eye and the operated one in terms of palpebral aperture, horizontal fissure and exophthalmometry result. After calculating these differences, we averaged them and compared the cases of natural hydroxyapatite implants with acrylic ones. Within the studied sample, the difference between the palpebral aperture of the operated eye and the healthy one has an average of 0.90 in the case of natural hydroxyapatite implants and 2.70 in the case of acrylic implants. Through the t-test for independent samples, it was observed that there is a statistically significant difference between the difference in apertures of the operated eye and the healthy one in hydroxyapatite implants compared to acrylic ones. We can state that in the case of acrylic implants the difference between the apertures of the operated and healthy eye is significantly greater than in the case of natural hydroxyapatite implants.
The average difference between the healthy and the operated eye in the horizontal fissure in the case of the natural hydroxyapatite implant was 1.90, while in the case of the acrylic implants it was 2.86. The result of the t-test for independent samples showed that the average difference between the healthy and the operated eye in the horizontal fissure in the case of the natural hydroxyapatite implant differs statistically significantly from the average difference between the healthy and the operated eye in the horizontal fissure in the case of the acrylic implants (t=-2.404; df=41; p=0.021). Therefore, we can state that in the cases of the natural hydroxyapatite implants, the horizontal fissure of the operated eye is much closer to the horizontal fissure of the healthy eye than in the case of the acrylic implants. We proceeded identically as in the previous cases to determine the differences between the two types of implants regarding the exophthalmometry result. The average difference between the healthy and the operated eye The mean difference between the healthy and the operated eye of the exophthalmometry result in the case of the natural hydroxyapatite implant was 1.65, while in the case of the acrylic implants it was 3.87. Since p<α(0.001), with a probability of 95%, we can state that the difference in means is between -2.838 and -1.601, thus accepting the fact that the mean difference between the healthy and the operated eye of the exophthalmometry result in the case of the natural hydroxyapatite implant is significantly different from the mean difference between the healthy and the operated eye of the exophthalmometry result in the case of the acrylic implant.
Verification of objective 3: Existence of a correlation between age and the aesthetic appearance of the prosthetic eye 4 years after prosthetics
It is observed that there is a significant correlation between age, on the one hand, and the difference in aperture between the two eyes (rho=0.322, n=43, p=0.035) and the difference in the horizontal fissure between the two eyes, on the other hand (rho=0.503, n=43, p=0.001), which shows that as age increases, the differences between the healthy eye and the operated eye in terms of palpebral aperture and horizontal fissure become more pronounced. The same cannot be said about the results of exophthalmometry, the evolution of the differences between the two eyes not being necessarily related to age. Discussions The modification of the general appearance of the face occurs with advancing age through laxity of facial tissues and fat. A series of changes occur in the eyelids and orbit that contribute to the etiology of many eyelid conditions such as ectropion, entropion, dermatochalasis or blepharoptosis. These changes can affect the position of the eyelids, the eyeball or the eyebrows and surgical interventions can contribute to the final cosmetic appearance especially after evisceration and prosthetics of the anophthalmic cavity. The insufficient cavity syndrome described by Tyers and Collin2 characterized by a deep superior sulcus, enophthalmic appearance, ptosis of the upper eyelid and malposition of the lower eyelid that occurs especially in the case of insufficiently prosthetic cavities is almost a rule in the case of acrylic implants more than 4 years after prosthetics. Integrated implants, offering the advantage of motility, maintain normal anatomical ratios for longer, the changes occurring 4 years after prosthesis are minor. Since there is no data in the literature regarding the follow-up of these prostheses for a period longer than 4 years, we can say that the hydroxyapatite implant represents the best implantation alternative to date, although the premises of orbital fat loss and tissue laxity require the long-term reconsideration of an implant with adjustable size that could overcome this shortcoming. Conclusions The results obtained helped us to conclude the following:
- There are significant differences in the aesthetic appearance between the operated and healthy eye 4 years after the prosthesis;
- in the case of acrylic implants, the difference between the apertures of the operated and healthy eye is significantly greater than in the case of natural hydroxyapatite implants;
- in the case of natural hydroxyapatite implants, the horizontal fissure of the operated eye is much closer to the horizontal fissure of the healthy eye than in the case of acrylic implants;
- the average difference between the healthy and operated eye in the exophthalmometry result in the case of the natural hydroxyapatite implant is significantly different from the average difference between the healthy and operated eye in the exophthalmometry result in the case of the acrylic implant;
- It is observed that there is a significant correlation between age, on the one hand, and the difference in aperture between the two eyes and the difference in the horizontal fissure between the two eyes, on the other hand, which shows that as we age, the differences between the healthy eye and the operated eye in terms of the palpebral aperture and the horizontal fissure become more pronounced. The same cannot be said about the results of exophthalmometry, the evolution of the differences between the two eyes not being necessarily related to age.
- The hydroxyapatite implant represents the best implantation alternative to date, although the premises of orbital fat loss and tissue laxity require the long-term reconsideration of an implant with adjustable size that could overcome this shortcoming.
STUDY OF THE NANOSTRUCTURED HYDROXYAPATITE IMPLANT IN THE EVISTICATED ANIMAL MODEL
Objectives: In this study, we aimed to investigate as the main objective the biocompatibility of an implant with expandable potential made of nanostructured hydroxyapatite (produced by the National Institute of Rare and Non-Ferrous Materials, Bucharest) implanted in the eviscerated animal model on the globe and as a secondary objective the proliferation rate of fibrovascular tissue within the implant. Nanocomposite materials The hybrid systems studied in this work were obtained by the hydrothermal method as an innovative technique for obtaining organic-inorganic hybrid materials [patent application no. A200500313, authors Roxana M. Piticescu, G. C. Chiţanu, M. Albulescu, R. M. Negriu]. Hydrothermal synthesis was carried out at low temperatures (T < 1200C) and high pressures given by autogenous pressure and external pressure introduced into the system3-7. Surgical intervention methodology: The animals used were weighed then general anesthesia was performed with Xylazine (Xilazin Bio, Maravet Animal Health) 0.15 ml/kgc administered intramuscularly, then after 10 minutes ketamine was administered intravenously (Ketaminol10, MSD Animal Health) at a dose of 0.1 lm/kgc. After the installation of general anesthesia, we performed the perilimbic conjunctival detachment on 3600, followed by the detachment of the Tenon capsule and radial keratotomy on 3600. We curetted the contents of the eyeball using the curette, removing the choroid, iris, lens, vitreous and retina. We cauterized the central retinal vein and artery after extracting 7 ml of uncoagulated blood from the scleral sac. We introduced 0.2 mg of nanostructured hydroxyapatite powder into the scleral sac. We sutured the sclera with separate threads leaving a space of about 2 mm for the injection of the mixture of nanostructured hydroxyapatite mixed with uncoagulated blood. The uncoagulated blood was mixed during the sclera suture by adding 0.3 mg of nanostructured powder to 4.5 ml of serum, obtaining a volume of 5 ml of product. This was injected into the sutured scleral sac using a syringe, thus introducing the 5 ml of powder mixed with blood. The sclera and then the Tenon capsule were sutured with 5-0 absorbable thread. The conjunctival suture was performed with 8-0 non-absorbable threads. Local antibiotic ointment (Tobrex, ophthalmic ointment, Alcon) was applied and a first dose of general antibiotic (Enrofloxacin-Ganadexil Enro 5%, Industrial Veterinaria SA 0.5 ml/kgb/day) was administered.
ResultsThe CT analysis performed one month and two months postoperatively has the following values in Hounsfield units, presented in table 2
Maximum density of hydroxyapatite implant at 1 month postoperatively (HU)Maximum density of hydroxyapatite implant at 2 months postoperatively (HU)Normal orbital bone density (HU)Rabbit 1400629989Rabbit 23505891008Rabbit 34305881200Rabbit 4260498970Table 2: density of hydroxyapatite implant measured at CT examination in Hounsfield units
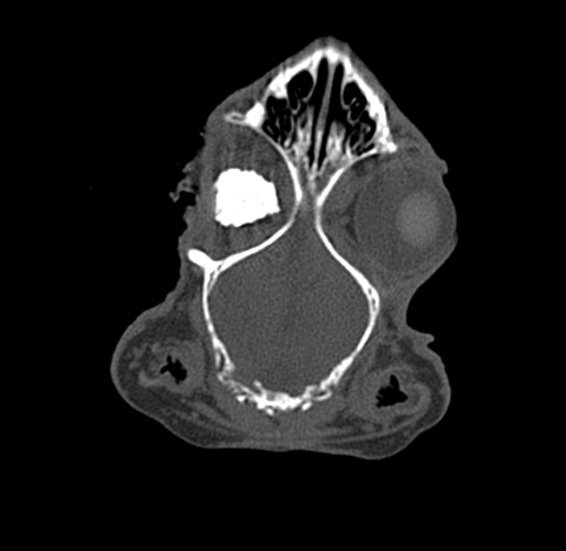
Figure 10: Hydroxyapatite implant – coronal section CT appearance at 1 month postoperatively. Increased bone density is noted inside the implant, but inhomogeneous, with areas of fibrovascular tissue
The histolopathological analysis performed shows in the meshes of the prosthetic material, fibrovascular tissue and minimal polymorphic inflammatory infiltrate (lymphocytes, plasma cells and polymorphonuclear neutrophils) and moderately frequent multinucleated giant cells of the “foreign body” type at the interface with the hydroxyapatite as well as osteoclasts at the interface with the hydroxyapatite nanocomposite material. At different levels in the muscle tissue and in the corresponding sclera, amorphous, acellular material (mono and multifilament surgical threads) bordered by multinucleated giant cells of the “foreign body” type is observed. (Figure 11,12). It can be observed that the invasion of the implant with fibrovascular material begins from the incision and the initial suture area, and the presence of multinucleated giant cells of the foreign body type in not very large numbers attests to good compatibility, at least equal to that of the suture material.
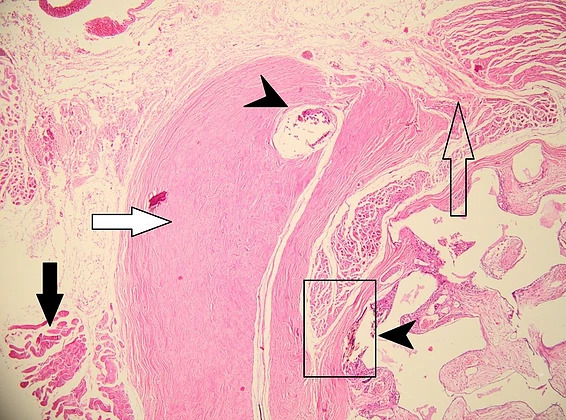
Figure 11: Histopathological appearance of the hydroxyapatite implant in hematoxylin-eosin (HE) staining – subject 1. The following structures are depicted: black arrow – striated muscle, white arrow – remnant sclera, empty arrow – incision site, arrowhead – surgical threads. Proliferation of fibrovascular tissue is observed inside the implant starting from the incision and suture site with uniform distribution through the nanostructured hydroxyapatite material (observed as white-gray areas marked by blue arrows). The fibrovascular tissue present attests to the complete vascularization of the implant 2 months after implantation with good tolerability.
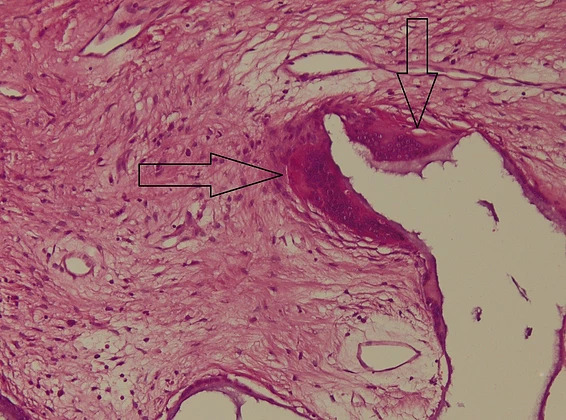
Figure 12: Histopathological appearance of the hydroxyapatite implant in hematoxylin-eosin (HE) staining – subject 2. Marked with arrows are the osteoclasts at the interface with the nanostructured hydroxyapatite material. The presence of osteoclasts attests to the tendency of hydroxyapatite degradation necessary for the formation of new bone tissue.
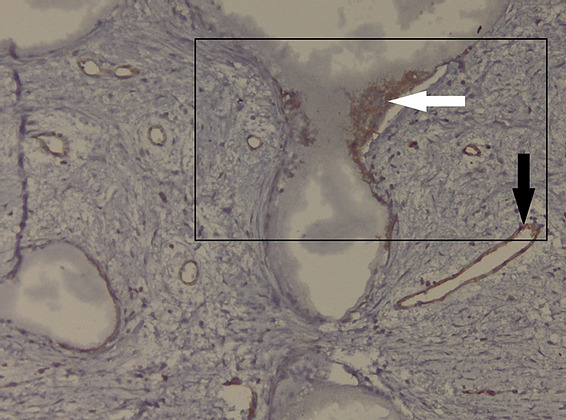
Figure 13: Microscopic appearance of the implant – CD31 immunohistochemical staining. The presence of CD31 + osteoclasts at the level of the implant meshes (black frame) of hydroxyapatite (white arrow) and the presence of CD31 + vascular endothelium (black arrow) is noted;
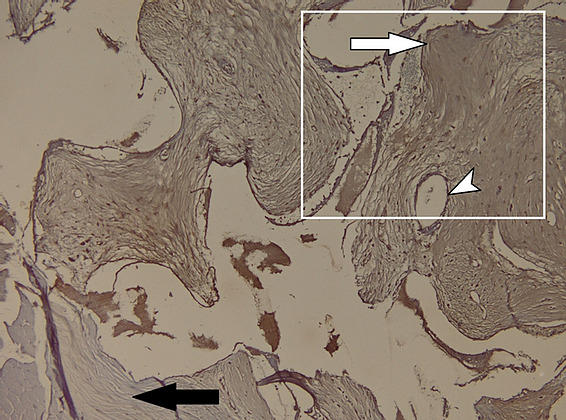
Figure 14: Microscopic appearance of the hydroxyapatite implant in CD34 immunohistochemical staining. The muscle tissue is negative for CD34 (black arrow), the presence of vascular endothelium as a positive internal control (white arrowhead) and fibroblasts, positive for CD34, at the level of the prosthetic material – hydroxyapatite (white arrow);
Discussions CT analysis performed one month postoperatively shows nanostructured hydroxyapatite density values in the scleral sac lower than the bone density of the animal model, but progressively increases at 2 months postoperatively. In terms of density, this is above the density of fibrous tissue but below the bone density of the animal model. In a study published by Froum et al., where a sinus allograft was implanted in humans and allowed to heal, it was demonstrated that a bone volume of about 25% of normal bone volume is sufficient to support a titanium implant8. In the study we found a progressive increase as healing progresses with a maturation of the newly formed tissue from type 2 bone density (300-500 HU) to type 1 bone density (over 500 HU). Histopathological analysis shows bone tissue formation inside the implant, the presence of fibrovascular tissue but also inflammatory cells. Also, the large number of osteoclasts is a marker of the degradation of nanostructured hydroxyapatite in the local production of new bone. Considering the existence of an extensive infectious process in one of the subjects that required the administration of general and local antibiotics for a longer period, the presence of inflammatory tissue rich in polymorphonuclear cells and lymphocytes is a valuable marker of the existence of this complication. However, it is known that inflammatory tissue transforms over time, after the resolution of the infection, into fibrous, scar tissue, which for this type of implant does not constitute a disadvantage, it can only be considered the possibility that the fibrosis process inside the implant may last longer. Conclusions: The progressive increase in the formation of fibrous tissue and new bone as healing progresses with a maturation of the newly formed tissue from type 2 bone tissue (300-500 HU) to type 1 bone tissue (over 500 HU) argues for the possibility of adapting a rapid dowel and screw to the animal model. In addition, histological analysis of the newly formed tissue inside the scleral sac reveals the rapid formation of bone and osteoid material alongside fibrovascular tissue, which is an important premise in promoting nanostructured hydroxyapatite materials in the prosthesis of the anophthalmic cavity. Moreover, the presence of CD31 and CD34 positive cells argues for rapid angiogenesis and fibrogenesis.
STUDY OF THE NANOSTRUCTURED HYDROXYAPATITE IMPLANT FOR PROSTHESIS IN CASE OF FRACTURES OF THE LOWER WALL AND LOWER MARGIN OF THE ORBIT IN ANIMAL MODEL
Objective: In this study, we aimed as the main objective to integrate a preformed implant of nanostructured hydroxyapatite (produced by the National Institute of Rare and Non-Ferrous Materials, Bucharest) implanted in the animal model on a defect of the lower orbital wall (floor) and the lower rim of the orbit and as a secondary objective the proliferation rate of fibrovascular tissue within the implant.Material and method: Nanostructured materialThe nanostructured systems studied in this work were obtained by the hydrothermal method as an innovative technique for obtaining organic-inorganic materials [patent application no. A200500313, authors Roxana M. Piticescu, G. C. Chiţanu, M. Albulescu, R. M. Negriu]. Hydrothermal synthesis was carried out at low temperatures (T = 8000C) and high pressures (P = 1 t) for 30 minutes, given by the autogenous pressure and the external pressure introduced into the system3-7. The preformed implant was made in a round shape with a diameter of 0.4 cm and upon implantation, 2 grooves were made on its surface for the passage of a 5-0 absorbable thread for attachment to the periosteum. Surgical intervention methodology: The animals used were weighed, then general anesthesia was performed with Xylazine (Xilazin Bio, Maravet Animal Health) 0.15 ml/kgb administered intramuscularly, then after 10 minutes, ketamine was administered intravenously (Ketaminol10, MSD Animal Health) at a dose of 0.1 ml/kgb. We administered 0.15 ml of adrenaline 1/100,000 in the lateral canthus and in the bottom of the inferior conjunctival sac for good local hemostasis. After the installation of general anesthesia, we performed a lateral canthotomy and cantholysis and for better visualization of the inferior wall, we placed a 4.0 silk traction thread through the lower eyelid. We performed the conjunctival incision at the level of the inferior fornix and the dissection in the plane between the orbicularis muscle and the orbital septum towards the inferior edge of the orbit. We opened the orbital septum and lifted the orbital periosteum from the level of the inferior edge of the orbit. Using a trephine attached to a dental micromotor, we created a defect in the inferior orbital wall of approximately 0.5 mm in diameter. We placed the hydroxyapatite implant in the preformed defect and sutured the resorbable threads to the bone periosteum. The residual defect of approximately 0.1 mm was filled with nanostructured hydroxyapatite powder. We sutured the periosteum and closed the orbital septum with 8.0 absorbable sutures. We sutured the conjunctiva with separate 8.0 absorbable sutures and sutured the lateral canthus with 6.0 non-absorbable sutures. We applied 0.3% tobramycin and 0.1% dexamethasone ointment (Tobradex, ung.oft, Alcon) and administered a dose of enrofloxacin (Ganadexil Enro 5%, Industrial Veterinaria SA) 0.5 ml/kg/day.

(b)

(a)

(d)

(c)C
Figure 15: Intraoperative aspect (a) transconjunctival approach and lateral canthotomy allow easy lift to the periosteum of the inferior orbital rim (b) a defect is made in the inferior orbital wall and orbital rim of 0.5 cm (white arrow) (c) the hydroxyapatite and polyurethane implant is placed in the orbital floor defect and sutured to the periosteum (blue arrow) (d) it is covered with nanostructured hydroxyapatite powder.
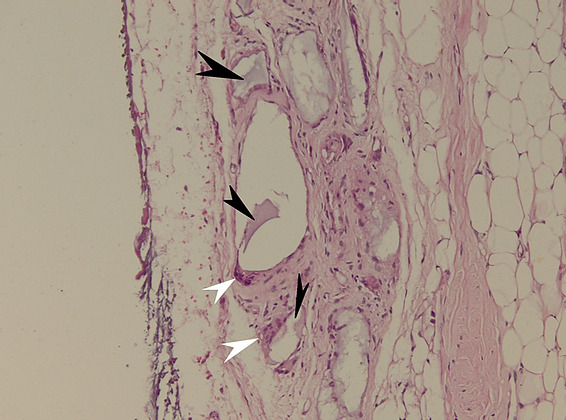
Figure 16: Microscopic appearance of the implant in HE X 200 staining. The presence of osteoclasts (white arrowhead) rich in mitochondria and with large nuclei – a sign of activity, at the interface with hydroxyapatite (black arrowhead) is noted.
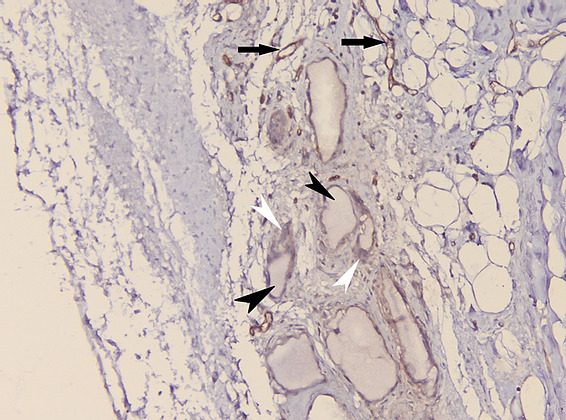
Figure 17: Appearance of the hydroxyapatite implant in CD31 immunohistochemical staining. The presence of hydroxyapatite crystals at the level of the bone defect (black arrowheads) and osteoclasts – positive for CD31 (white arrowheads) is noted. As an internal control, the presence of vascular endothelium positive for CD31 (black arrows) is observed.
DiscussionsThe CT analysis performed one month postoperatively shows values of the density of the hybrid nanostructured hydroxyapatite implant at the level of the bone defect lower than the bone density of the animal model, but they increase progressively at 2 months postoperatively. In terms of density, this is above the density of fibrous tissue but below the bone density of the animal model. The nanostructured hydroxyapatite implant at 1 month postoperatively presents good density but in two cases the persistence of a cleavage plane between the implant and the bone is noted, demonstrated by the presence of a fibrovascular tissue with low density (HU=40). In one subject the presence of a large cleavage plane is observed, the explanation of this phenomenon could be related to the large difference between the density of the fibrovascular tissue and the density of the bone cortex (HU=1120) which makes the visibility of the fibrovascular tissue interpreted as a lack of substance. The nanostructured hydroxyapatite implant at 2 months postoperatively presents on CT examination a density closer to the bone density of the animal model and the absence in most cases of the cleavage plane, a clear sign of the integration of the implant into the bone tissue.
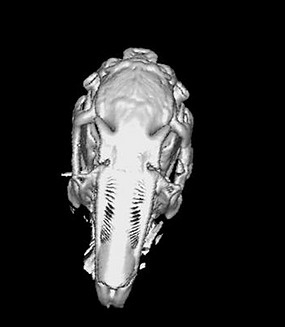
Figure 18: Rabbit1-3D CT bone reconstruction. Nanostructured hydroxyapatite implant at 1 month postoperatively (arrow). The persistence of a cleavage plane between the implant and the bone is noted, demonstrated by the presence of a low-density fibrovascular tissue (HU=40)
Conclusions: Analysis of the preformed nanostructured hydroxyapatite implant with application in orbital fractures by CT examination performed at 1 month postoperatively shows values of the density of the hybrid nanostructured hydroxyapatite implant at the level of the bone defect lower than the bone density of the animal model, but which progressively increase at 2 months postoperatively. The integration of the nanostructured implant is good, the coverage of the bone defect being complete. In addition, histological and CD31 immunohistochemical analysis shows development of fibrous tissue around the bone defect and good implant integration. Preformed nanostructured hydroxyapatite implants may represent an alternative to existing implants for the prosthesis of orbital wall fractures.
FINAL CONCLUSIONS
The evaluation of the results obtained in the 5 studies conducted, 3 clinical and 2 preclinical on animal models allowed me to conclude the following:
- In the study of integrated and non-integrated implants in eviscerated patients, there is no statistically significant relationship between the type of implant used and the occurrence of a certain type of complication. Although it is observed that dehiscence occurred only in the cases of hydroxyapatite implants, the very small number of cases prevents us from showing that this type of complication occurs more frequently in the case of these implants. The explanation is related to the fact that placement in the scleral sac offers better resistance to infection, extrusion and dehiscence. On the other hand, there is a large number of associated complications – infection followed by extrusion which gives additional gravity to these types of complications, which occur more frequently in the case of acrylic and silicone implants.
- In the study of integrated and non-integrated implants in enucleated patients, it is observed that dehiscence occurs only in the cases of hydroxyapatite implants, but their number is small, while extrusion cases occur in an overwhelming proportion only in the case of acrylic and silicone implants. We can conclude that integrated hydroxyapatite implants, either ready-mixed or preoperatively shrunk, allow better integration of the prosthesis compared to non-integrated implants, thus being preferred in the case of enucleated patients.
- If we analyze the aesthetic appearance of the operated eye compared to the healthy eye in enucleated patients, in the case of acrylic implants, the difference between the apertures of the operated and healthy eye is significantly greater than in the case of natural hydroxyapatite implants, similarly in the case of natural hydroxyapatite implants, the horizontal fissure of the operated eye is much closer to the horizontal fissure of the healthy eye, than in the case of acrylic implants. In addition, we analyzed the impact of age on the prosthetic eye and the healthy eye, where we found statistically significant differences, which shows that as we age, the differences between the healthy and the operated eye in terms of palpebral aperture and horizontal fissure become more pronounced. We can conclude that the superior motility of integrated implants allows the natural appearance of the operated eye to be preserved and that the natural changes that occur due to age are more pronounced in the case of acrylic implants.
- Also from an aesthetic point of view, the exophthalmometry analysis, where in the case of the natural hydroxyapatite implant the average difference between the healthy and the operated eye is small, reveals in patients with acrylic implants a greater difference between the operated and the healthy eye, arguing for the existence of a higher degree of enophthalmia in non-integrated implants 4 years after implantation.
The conclusions of the clinical studies made me look for answers to the problems raised, namely:
- The creation of an integrated implant (hydroxyapatite has so far presented an alternative with excellent biocompatibility) that will allow adjustments from an aesthetic point of view so that the shortcomings related to the aperture and height of the palpebral fissure are as small as possible or even absent. The degree of enophthalmia could also be controlled by the progressive injection of a mixture of hydroxyapatite powder and blood to enlarge the implant as orbital fat atrophy occurs.
- Since hydroxyapatite is a material with good compatibility, I wanted to create an implant with a high healing and proliferation rate so that the waiting time required for the final prosthesis is shortened, for this reason the proposal of hydroxyapatite-based nanomaterials that offer a large contact surface with living cells with proliferation potential within the high implant.
- The lack of an ideal implant for orbital wall fractures led me to investigate the possible rapid osseointegration of a preformed nanostructured hydroxyapatite implant.
Thus, from the two preclinical studies on animal models, the following conclusions can be drawn:
- In the study of the nanostructured hydroxyapatite powder implant in an eviscerated animal model, we discovered a progressive increase in the formation of fibrous tissue and new bone as healing progresses with a maturation of the newly formed tissue from type 2 bone tissue (300-500 HU) to type 1 bone tissue (over 500 HU). This argues for the possibility of adapting a rapid dowel and screw to the animal model. In addition, histological analysis of the newly formed tissue inside the scleral sac reveals the rapid formation of bone and osteoid material alongside fibrovascular tissue, which is an important premise in promoting nanostructured hydroxyapatite materials in the prosthesis of the anophthalmic cavity. Moreover, the presence of CD31 and CD34 positive cells argues for rapid angiogenesis and fibrogenesis. The adjustable nanostructured hydroxyapatite implant is a promising alternative for patients who undergo evisceration or enucleation, but further research and large-scale studies are needed.
- In the study of the preformed nanostructured hydroxyapatite implant applied in orbital fractures, the CT analysis performed one month postoperatively shows values of the density of the hybrid nanostructured hydroxyapatite implant at the level of the bone defect lower than the bone density of the animal model, but which progressively increase at 2 months postoperatively. The integration of the nanostructured implant is good, with complete coverage of the bone defect. In addition, the histological analysis shows the development of fibrous tissue around the bone defect and good implant integration. Preformed implants of nanostructured hydroxyapatite can represent an alternative to existing implants for the prosthesis of orbital wall fractures, while also being cost-effective, with the creation of personalized implants being possible by using CT reconstruction images and the creation of the personalized implant through 3D printing.
The proposal of this doctoral thesis to find new ways of oculo-orbital reconstruction can be taken further by improving the proposed implants and conducting phase II and III studies for immediate medical applicability.
Bibliography:
- Shields CL, Shields JA, De Potter P, Singh AD. Problems with the hydroxyapatite orbital implant: experience with 250 consecutive cases. Br J Ophthalmol. 1994; 78(9): 702-6.
- Tyers AG, Collin JR. Orbital implants and post enucleation socket syndrome. Trans Ophthalmol Soc U K. 1982; 102 (Pt 1): 90-2.
- Popescu LM, Piticescu RM, Rusti CF, Maly M, Danani A, Kintzios S, et al. Preparation and characterization of new hybrid nanostructured thin films for biosensors design. Materials Letters. 2011; 65(13): 2032-5.
- Piticescu RM, Popescu LM, Buruiana T. Composites containing hydroxyapatite and polyurethane ionomers as bone substitution materials. Dig J Nano Bio. 2012; 7: 477-85.
- Vasile E, Popescu L, Piticescu R, Burlacu A, Buruiana T. Physico-chemical and biocompatible properties of hydroxyapatite based composites prepared by an innovative synthesis route. Materials Letters. 2012; 79: 85-8.
- Piticescu RM, Vilarnho P, Popescu L, Piticescu RR. Hydrothermal synthesis of perovskite based materials for microelectronic applications. Journal of optoelectronics and advanced materials. 2006; 8(2): 543.
- Piticescu RM, Chitanu GC, Meghea A, Giurginca M, Negroiu G, Popescu LM. Comparative study of in situ interactions between maleic anhydride based copolymers with hydroxyl apatite. Key Engineering Materials. 2008; 361: 387-90.
- Froum SJ, Tarnow DP, Wallace SS.The use of mineralized allograft for sinus augmentation: An interim histological casereport from a prospective clinical study.Compendium. 2005;26:259-268.
- Beuerman RW, Pedroza L. Ultrastructure of the human cornea. Microsc Res Tech. 1996; 33(4): 320-35.
- Doughty MJ, Seabert W, Bergmanson JP, Blocker Y. A descriptive and quantitative study of the keratocytes of the corneal stroma of albino rabbits using transmission electron microscopy. Tissue Cell. 2001; 33(4): 408-22.
- Poukens V, Glasgow BJ, Demer JL. Nonvascular contractile cells in sclera and choroid of humans and monkeys. Invest Ophthalmol Vis Sci. 1998; 39(10): 1765-74.
- Freddo TF. Ultrastructure of the iris. Microsc Res Tech. 1996; 33(5): 369-89.
- Castro-Correia J. Understanding the choroid. Int Ophthalmol. 1995; 19(3): 135-47.
- Smelser GK. Electron microscopy of a typical epithelial cell and of the normal human ciliary process. Trans Am Acad Ophthalmol Otolaryngol. 1966; 70(5): 738-54.
- Bill A, Sperber G, Ujiie K. Physiology of the choroidal vascular bed. Int Ophthalmol. 1983; 6(2): 101-7.
- Hayreh SS. In vivo choroidal circulation and its watershed zones. Eye (Lond). 1990; 4 ( Pt 2): 273-89.
- Lee SC, Lee I, Koh HJ, Kim SH, Kwon OW. Massive suprachoroidal hemorrhage with retinal and vitreous incarceration; a vitreoretinal surgical approach. Korean J Ophthalmol. 2000; 14(1): 41-4.
- Hollenberg MJ, Burt WL. The fine structure of Bruch’s membrane in the human eye. Canadian journal of ophthalmology Journal canadien d’ophtalmologie. 1969; 4(3): 296-306.
- Curcio CA, Allen KA. Topography of ganglion cells in human retina. The Journal of comparative neurology. 1990; 300(1): 5-25.
- Dumitrache M, Anitescu M, Carstocea B. [Laser treatment in diabetic retinopathy]. Oftalmologia. 1995; 39(2): 159-69.
- 21. Dumitrache M, Anitescu M, Gheorghe L. [The morphological substrate and histogenesis of systemic and ocular atherosclerosis]. Oftalmologia. 1995; 39(1): 11-7.
- Popa DP, Tacorian D, Dumitrache M. [Atherosclerosis and retinal detachment]. Rev Chir Oncol Radiol O R L Oftalmol Stomatol Ser Oftalmol. 1978; 22(1): 11-4.
- Pop DPD, Dumitrache M, Gavan G. [Obstructive retinal lesions]. Rev Chir Oncol Radiol O R L Oftalmol Stomatol Ser Oftalmol. 1985; 29(2): 81-6.
- Harman A, Abrahams B, Moore S, Hoskins R. Neuronal density in the human retinal ganglion cell layer from 16-77 years. The Anatomical record. 2000; 260(2): 124-31.
- Brubaker RF, Nagataki S, Townsend DJ, Burns RR, Higgins RG, Wentworth W. The effect of age on aqueous humor formation in man. Ophthalmology. 1981; 88(3): 283-8.
- American Academy of Ophthalmology. Anterior Segment Panel. Cataract in the adult eye. San Francisco: American Academy of Ophthalmology; 2001.
- Dumitrache M, Ciocalteu AM. [Congenital anomalies of the vitreous body]. Oftalmologia. 2010; 54(2): 3-6.
- Potop V, Dumitrache M. [Principles of treatment in ocular burns regarding the ocular surface and limbal stem cells]. Oftalmologia. 2005; 49(2): 27-34.
- Potop V, Dumitrache M, Ciocalteu A. The surface of the eye–a superficial entity with deep repercussions. J Med Life. 2009; 2(1): 66-71.
- Sellheyer K, Spitznas M. Ultrastructural observations on the development of the human conjunctival epithelium. Graefe’s archive for clinical and experimental ophthalmology. 1988; 226(5): 489-99.
- Steuhl K-P. Ultrastructure of the conjunctival epithelium. Developments in ophthalmology. 1988; 19: 1-104.
- 32. Watson PG, Young RD. Scleral structure, organisation and disease. A review. Experimental eye research. 2004; 78(3): 609-23.
- Price KM, Gupta PK, Woodward JA, Stinnett SS, Murchison AP. Eyebrow and eyelid dimensions: an anthropometric analysis of African Americans and Caucasians. Plastic and reconstructive surgery. 2009; 124(2): 615-23.
- Jones LT. An anatomical approach to problems of the eyelids and lacrimal apparatus. Archives of ophthalmology. 1961; 66(1): 111-24.
- American Academy of Ophthalmology. Pediatric Ophthalmology Panel. Esotropia and exotropia.
- Wright KW, Spiegel PH. Pediatric ophthalmology and strabismus: Springer; 2003.
- Iinuma T, Hirota Y, Ishio K. Orbital wall fractures. Conventional views and CT. Rhinology. 1994; 32(2): 81-3.
- Kim SH, Ahn KJ, Lee JM, Choi KH, Han SH. The usefulness of orbital lines in detecting blow-out fracture on plain radiography. Br J Radiol. 2000; 73(876): 1265-9.
- Ballinger PW, Frank ED, Merrill V. Merrill’s atlas of radiographic positions & radiologic procedures. 10th ed. St. Louis, Mo.: Mosby; 2003.
- Merrill V. Atlas of roentgenographic positions and standard radiologic procedures. 4th ed. Saint Louis: Mosby; 1975.
- Rao VM, Sharma D, Madan A. Imaging of frontal sinus disease: concepts, interpretation, and technology. Otolaryngol Clin North Am. 2001; 34(1): 23-39.
- Rao VM, el-Noueam KI. Sinonasal imaging. Anatomy and pathology. Radiol Clin North Am. 1998; 36(5): 921-39, vi.
- Rao VM, Levin DC. Turf wars in radiology: the past, present, and future importance of training standards in imaging. J Am Coll Radiol. 2005; 2(7): 602-6.
- Yanagisawa E, Smith HW, Thaler S. Radiographic anatomy of the paranasal sinuses. II. Lateral view. Arch Otolaryngol. 1968; 87(2): 196-209.
- Unni K. Nair AJA, Emmett T. Cunningham Jr. Ophthalmic Pearls: Trauma Identifying Intraocular Foreign Bodies. American Academy of Ophthalmology Web Site: wwwaaoorg 2007 [cited 2007 2007]; Available from:
- Gawler J, Sanders MD, Bull JW, du Boulay G, Marshall J. Computer assisted tomography in orbital disease. Br J Ophthalmol. 1974; 58(6): 571-87.
- Totir M, Ciuluvică, R., Dinu,I., Careba,I., Grădinaru,S. biomaterials for orbital fractures repair. Journal of Medicine and Life. 2014; 7(4): 59-62.
- Balta F, Gradinaru S, Ungureanu E, Ciuluvica R. BIOMATERIALS IN OPHTHALMOLOGY: HYDROXYAPATITE INTEGRATED ORBITAL IMPLANT AND NON-INTEGRATED IMPLANTS IN ENUCLEATED PATIENTS. Metalurgia International. 2013; 18(8).
- Gradinaru S, Totir M. , Iancu ,R. ,Leasu , C., Pricopie, S., Yasin ,S., Ciuluvică,R., Ungureanu ,E. Topographic measurements of eyelids and orbit in enucleated eyes with hydroxyapatite integrated implant versus PMMA implant Journal of Medicine and Life. 2014; 7(4): 71-4.
- Gradinaru S, Popescu V, Leasu C, Pricopie S, Yasin S ,Ciuluvică R, Ungureanu E Hydroxyapatite ocular implant and non-integrated implants in eviscerated patients Journal of Medicine and Life.2015 8(1)
